What’s the Deal with Vitamin D & COVID?
- Vitamin D deficiency has been proposed to play a role in risk of SARS-CoV-2 infection and/or risk or worse outcomes from COVID-19.
- Vitamin D supplementation has also been explored as a potential adjunct treatment for those with severe COVID-19 infection.
- Previously, vitamin D supplementation has been suggested to have some benefit against acute respiratory infections generally.
But what can we conclude based on current evidence?
This Sigma Statement will attempt to summarize the available evidence regarding how the risk of COVID-19 infection and mortality is potentially impacted by:
- Vitamin D status
- Vitamin D genotypes
- Vitamin D supplementation
Table of Contents
Introduction: COVID & Preventative Measures
Coronavirus disease (COVID-19) is a respiratory and systemic disorder caused by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) or novel Coronavirus (nCoV). Much is still unknown about SARS viruses, but SARS-CoV-2 spreads faster and farther than the 2003 SARS-CoV-1 virus. This is likely because of how easily it is transmitted from person to person, even from asymptomatic carriers of the virus.
At present (January 2022), there is no scientifically approved curative treatment for the virus; as a result, prevention remains to be the best strategy to combat infection. To this point a set of preventative measures recommended by the WHO to prevent infection and slow transmission endorsed worldwide by most governments and public health agencies, with varying levels of compliance by the general population. Such measures include:
- vaccination
- physical distancing
- mask wearing
- practicing good hygiene
- if unwell, to self-isolate until recovered
Beyond this, additional preventative and therapeutic measures have been explored, to reduce the risk of infection but also to reduce the severity of symptoms in those who do contract the virus. Vitamin D deficiency has been proposed to play a role in coronavirus infection (e.g. here and here). In addition, vitamin D supplementation has been explored as a potential adjunct treatment for those with severe COVID-19 infection, i.e., requiring hospitalisation, intensive care unit (ICU) admission and/or those requiring oxygen support.
In the decade preceding the coronavirus pandemic, a meta-analysis of randomised controlled trials (RCTs) reported protective effects of vitamin D supplementation against acute respiratory infections (ARIs). However, the effects are modest and there is a lack of homogeneity (the similarity of the results of studies included) across studies.
This Sigma Statement aims to summarize the available evidence regarding how the risk of COVID-19 infection and mortality is potentially impacted by vitamin D status, vitamin D genotypes, and vitamin D supplementation.
Key Definitions (click/tap to open)
Some terms you may encounter in this Statement and/or related reading:
“Mendelian randomization”: is a method in genetic epidemiology which uses genetic variants reliably associated with exposures of interest to estimate causal associations between a given biomarker, such as vitamin D, and disease.
“SARS-COV-2”: Severe Acute Respiratory Syndrome is a viral respiratory disease caused by a SARS-associated coronavirus. It is an airborne virus and can spread through small droplets of saliva in a similar way to the cold and influenza.
“asymptomatic carriers”: Asymptomatic carriers are those who never experience symptoms despite being infected.
“enveloped viruses”: A virus that has an outer wrapping or envelope. This envelope comes from the infected cell, or host, in a process called “budding off.” During the budding process, newly formed virus particles become “enveloped” or wrapped in an outer coat that is made from a small piece of the cell’s plasma membrane. The envelope may play a role in helping a virus survive and infect other cells.
“food fortification”: the practice of adding vitamins and minerals to commonly consumed foods during processing to increase their nutritional value.
Comparison to Other Coronaviruses
Coronaviruses are a family of enveloped RNA viruses broadly distributed in humans and animals that cause acute and chronic diseases. SARS-CoV-2 is the seventh human coronavirus to be identified. Of the six coronavirus species previously known to cause human diseases, four typically cause common cold symptoms. However, the other two , namely SARS- and MERS- (Middle East respiratory syndrome) coronavirus, can cause fatal respiratory disease.
With this latest coronavirus, SARS-CoV-2, infection can remain asymptomatic or cause modest symptoms. Severely sick patients require hospital admission and about 20 % of hospitalized patients will develop Acute Respiratory Distress Syndrome (ARDS) and require intensive care unit (ICU) treatment. A certain percentage of cases will also be fatal, with estimates of both the case fatality rate and crude mortality rate varying by location, time, and other factors. Currently case fatality rate estimates vary by country from 0.35 – 2.75%, with a world wide average of 1.8%. However, as put by Our World in Data, it is important to note that the case fatality rate “is the ratio between the number of confirmed deaths from the disease and the number of confirmed cases, not total cases. That means that it is not the same as – and, in fast-moving situations like COVID-19, probably not even very close to – the true risk for an infected person.”
Clinical Vulnerability and COVID-19
Since the beginning of the pandemic in early 2020, governments worldwide have responded with public health measures to protect the most vulnerable in society. Initially this focused on clinical vulnerabilities, as early data indicated that older adults, particularly those with poor health status or with dependencies and requiring institutional care, to be most vulnerable to COVID-19 death. As the pandemic continued into the first wave (February to August 2020), more data was generated to describe the profile of those most likely to experience severe COVID-19 infection, requiring hospitalisation, and potentially ICU care, and ultimately increasing risk of mortality. Those defined as ‘clinically extremely vulnerable’ to the virus included:
- people with respiratory conditions (severe asthma, COPD, bronchiectasis, and cystic fibrosis)
- compromised immune systems (such as those receiving treatment for cancer)
- older adults
- those with Class 3 obesity (defined as a body mass index of >40 kg/m2)
In addition to clinical vulnerability, it is now well established that those with lower socio-economic status are also at increased risk of COVID-19 infection and poorer outcomes. The risk factors for both severe coronavirus infection and vitamin D deficiency have many similarities, which has led researchers to investigate a potential relationship.
Vitamin D Physiology
Vitamin D is a precursor of the active form 1,25(OH)2D (calcitriol) and is present in two forms:
- Vitamin D3 (cholecalciferol)
- Vitamin D2 (ergocalciferol)
The main source in humans is via action of solar ultraviolet-B (UVB) radiation (270nm-300nm) on skin, converting 7-dehydrocholesterol (provitamin D3) into pre-vitamin D3, which is then rapidly converted to vitamin D3 as illustrated in the image below.
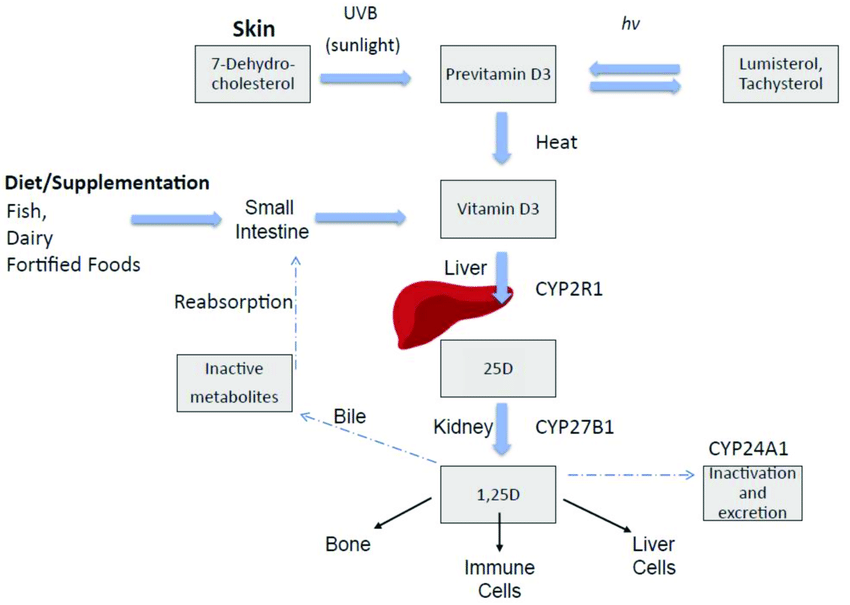
Vitamin D2 is produced via UVB radiation on plant sources such as mushrooms and yeast. Natural dietary sources of vitamin D3 are few, and include fish liver oils, oily fish, egg yolks and some fortified foods (e.g., some dairy and breakfast cereals) and supplements.
Irrespective of how it is acquired, vitamin D offers limited function until it has been activated, a process which requires two hydroxylation steps, as illustrated in the image above, namely:
- First, in the liver several enzymes but primarily vitamin D3 25-hydroxylase (CYP2RA), which converts it to the inactive precursor, 25-hydroxy vitamin D [25(OH)D]. This 25(OH)D is the prominent circulating form in humans and so it is the form that is measured to determine vitamin D status.
- The second hydroxylation step occurs in the tubular cells of the kidney, where the inactive 25(OH)D is converted to the biologically active metabolite 1, 25-dihydroxy vitamin D3 [1,25(OH)2D3], via the action of the enzyme 25vitamin D3-1α- hydroxylase (CYP27B1).
The active form of vitamin D, 1,25(OH)2D3, plays many important roles around the body, including modulating calcium and phosphate homeostasis. It is also present in many tissues including the kidneys, brain, immune cells, cardiovascular systems and pancreatic islets. Due to its ability to be synthesised endogenously, vitamin D is widely accepted to be a steroid hormone, as opposed to a vitamin by its classic definition.
Vitamin D Status and Risk Factors for Vitamin D Deficiency
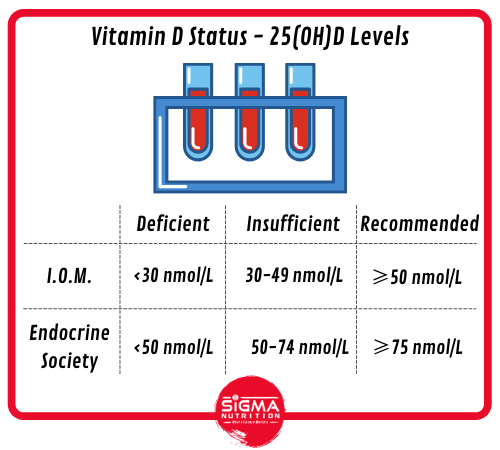
Serum 25(OH)D is accepted as the most accurate measure of vitamin D status, however, there is less agreement on how to define ‘deficiency‘ in the general population. Indeed, different groups provide different cut off points:
- The Institute of Medicine (IOM) advocate serum 25(OH)D concentrations ≥50nmol/L for bone health and consider levels <30 nmol/L to be deficient. The term ‘vitamin D insufficiency’ is used to describe serum levels of ≥30-50 nmol/L.
- In contrast, the Endocrine Society recommends serum 25(OH)D levels ≥ 75nmol/L to maximise an effect on bone and muscle metabolism. They deem vitamin D deficiency to be a 25(OH)D below 50 nmol/L (20 ng/ml), and vitamin D insufficiency as a 25(OH)D of 50–74 nmol/L (21–29 ng/ml).
Suboptimal levels of vitamin D are much more common than clinical toxicity, which is rare.
Several factors influence vitamin D status including:
- skin pigmentation
- use of sunscreen or concealing clothing
- season
- latitude
- being older or institutionalised
- obesity
- malabsorption
- renal and liver disease
- medication use
In general, UVB radiation on skin is the main source of vitamin D for humans. In countries north of the equator (40-60°N), vitamin D UVB doses are inadequate for 6 months of the year (October- March). The efficiency of UVB vitamin D production is reduced by as much as 50% in older adults compared to younger adults. This is due skin thinness, decreased skin integrity, and a reduction in transdermal cholesterol, that occures with advancing age. Additionally, there are also behavioural and social changes seen with advancing age that further limit vitamin D production, namely:
- Less time spent outdoors due to ill health or limited mobility (institutionalised or homebound)
- medication use (loop diuretics, statins, glucocorticoids)
- changes in body composition (increase in fat and decrease in muscle)
- sun avoidance (melanoma risk)
- reduced skin exposure (clothing and colder temperatures)
The striking overlap between risk factors for severe COVID-19 and vitamin D deficiency (i.e. older age, institulisatised adults, and those of black or Asian ethnic origin) has resulted in many researchers to hypothesise that vitamin D supplementation could provide opportunity as a preventative or therapeutic option for COVID-19.
Mechanistic Evidence for Vitamin D and COVID-19
From a mechanistic angle there is logic in exploring the potential for vitamin D metabolites to support innate antiviral effector mechanisms, in both:
- the early viraemic stages in SARS-COV-2
- later increased inflammatory phases of COVID-19
Vitamin D metabolites have long been known to support innate antiviral mechanisms (see here and here), including induction of antimicrobial peptides and autophagy. Of particular interest, vitamin D has important antiviral properties, including the induction of cathelicidin and b2-defensins synthesis, both of which have significant antibiotic and antiviral effects.
Chen and colleagues compared the clinical and immunological characteristics between moderate and severe COVID-19. They found that respiratory distress on admission is associated with unfavourable outcomes. Severe COVID-19 is associated with:
- increased cytokine levels (IL-6, IL-10, and TNF-α)
- lymphopenia (in CD4+ and CD8+ T cells)
- decreased IFN-γ expression in CD4+ T cells
Overall, this study characterized the ‘cytokine storm’ in severe COVID-19 and provided insights into immunotherapeutics and vaccine design. Recently, Adrian Martineau showed that airway diseases are associated with dysregulated vitamin D metabolism, raising the possibility that vitamin D deficiency may occur as a result of pulmonary inflammation.
Observational Studies of Vitamin D Status and COVID-19
Circulating levels of 25(OH)D and incidence and severity of COVID-19 have been explored by numerous investigators. Increased vitamin D levels have been proposed to protect against COVID-19 based on in vitro, observational, and ecological studies. Two ecological studies have reported inverse correlations between national estimates of vitamin D status and COVID-19 incidence and mortality in Europe. Mariani et al., utilised publicly available estimates of national prevalence of vitamin D deficiency (<50 mmol/l) across 46 countries and reported an association with risk of being infected with COVID-19, severity of the disease, and risk of death.
Another study in a single centre in the US, included 489 COVID-19 patients who had a measurement of 25(OH)D within 1 year of receiving a COVID-19 positive test. Vitamin D status was estimated based on ‘most likely deficient’ since previous analysis and COVID-19 testing. The study was one of a few that controlled for important confounders, such as sex, BMI, medical history, and race. “Likely deficient” vitamin D status was associated with increased COVID-19 risk (OR 1.77), in those who had not commenced vitamin D treatment since their previous diagnosis of deficiency (as reported on the hospital electronic system).
A study in Israel reported independent associations between low 25(OH)D levels (measured prior to the COVID-19 pandemic) and subsequent incidence and severity of COVID-19. This investigation is limited by the use of historic 25(OH)D measurements, which might not reflect circulating concentrations at the time of exposure to SARS-COV-2. On the other hand, a study in a northern Italy hospital found no association between vitamin D and COVID-19.
In a review article, researchers in Italy concluded that poor vitamin D status appears to be linked to an increased risk of SARS-CoV-2 infection, but age, sex, and comorbidities seem to play a more important role in COVID-19 severity and mortality. A different group of Italian researchers published an observational study of 324 patients with COVID-19 that found taking vitamin D supplements was not linked to risk of hospitalization but vitamin D deficiency was associated with a higher risk of dying if hospitalized.
Current evidence is encouraging but conflicting. As described above, vitamin D levels are associated with numerous confounding variables, and the associations may not be causal. Therefore to minimize bias due to confounding when considering this relationship, Mendelian Randomization (MR) studies may offer an important insight.
Mendelian Randomisation Studies: Vitamin D and COVID
Guillaume Butler-Laporte and collegues utilised a genome-wide association study (GWAS) of 443,734 participants of European ancestry (including 401,460 from the UK Biobank). The researchers did not observe evidence to support an association between 25(OH)D levels and COVID-19 susceptibility, severity, or hospitalization. Hence, vitamin D supplementation as a means of protecting against worsened COVID-19 outcomes was not supported by genetic evidence.
Similar was reported by Cui et al., who demonstrated that genetically lower serum 25(OH)D concentrations were not causally associated with COVID-19 susceptibility, severity or hospitalized traits.
In another study researchers conducted a regression analysis (a statistical method that basically shows the relationship between variables and the outcome of interest) to identify associations between vitamin D factors and COVID-19 (risk of infection, hospitalisation and death) in 417,342 participants from UK Biobank. Additionally, the authors performed a MR study to look for evidence of a causal effect. The main MR analysis did not show that genetically-predicted vitamin D levels are causally associated with COVID-19 risk (OR = 0.77, 95% CI 0.55–1.11, P = 0.160). Interestingly, the authors found no strong association between vitamin D levels and COVID-19 risk or severity after adjustment for confounders, results that are in accordance with other recently published evidence.
It is important to note that the vitamin D UK biobank samples were collected over a decade ago, and technique used (the DiaSorin immunoassay) is deemed inferior to other techniques, such as Liquid Chromatography with tandem Mass Spectrometry (LC-MS/MS). Furthermore, as the authors acknowledged, not all participants were tested for present (or past) COVID-19 infection; and so as it’s possible that some of the participants who were in the control group could have actually been previously asymptomatic infected individuals, this introduces a source of bias.
Vitamin D Supplement Use and COVID-19
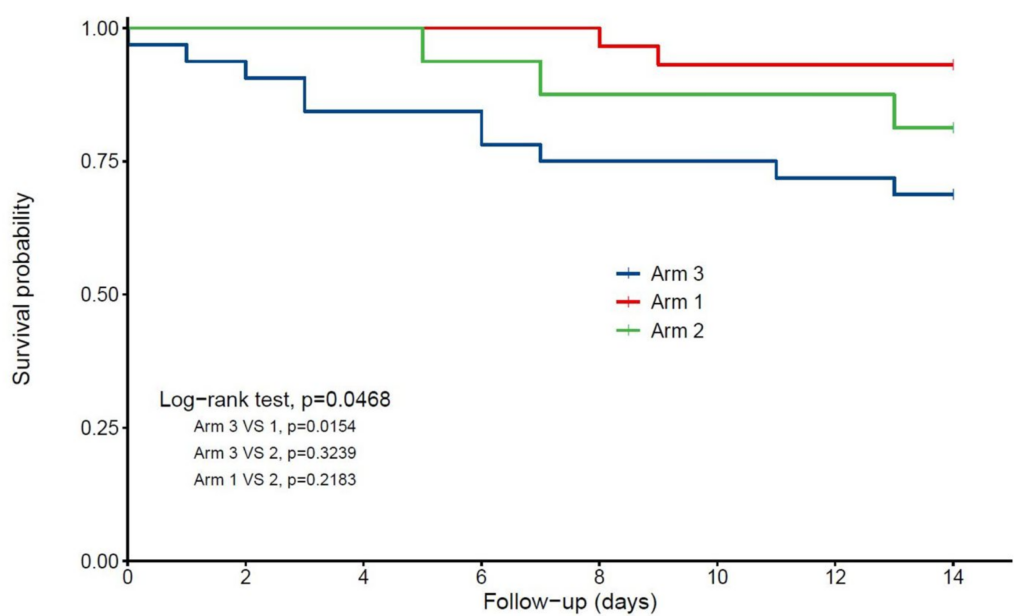
In a study investigating frail older in-patients with COVID-19, regular vitamin D supplement use in the year prior to a COVID-19 diagnosis was associated with less severe disease and better survival than taking no vitamin D or receiving supplementation shortly after diagnosis. Below is a figure from that study, showing Kaplan–Meier estimates of the cumulative probability of COVID-19 participants’ survival according to vitamin D interventions.
- Arm 1: regular vitamin D supplementation
- Arm 2: vitamin D supplementation initiated after COVID-19 diagnosis
- Arm 3: no vitamin D supplementation
Another study investigated the potential benefits of delivering a single high dose of vitamin D3 (200, 000 IU) in patients with moderate to severe COVID-19. The investigators determined that bolus doses of vitamin D did not significantly reduce hospital length of stay, as shown in the figure below.
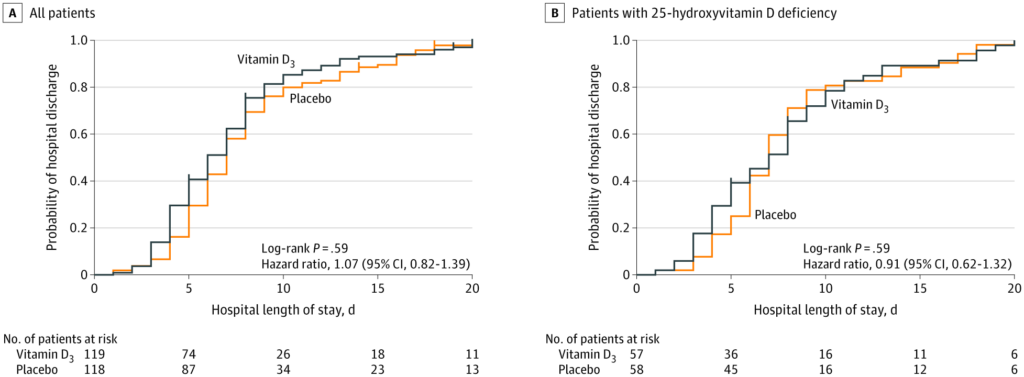
Copyright © 2021, American Medical Association
To date, RCTs administering bolus doses of vitamin D and various outcomes, continually fail to demonstrate beneficial effects. A pilot RCT of 76 in-patients with COVID-19 in Spain found that treatment with high-dose vitamin D (in combination with standard care of hydroxychloroquine and azithromycin), significantly reduced the risk of ICU admission. This was a parallel pilot randomized open label, double-masked clinical study aiming to assess whether vitamin D3 can reduce the need for admission to ICU, and related death. Serum 25(OH)D concentrations at baseline or during treatment are not available, and how baseline vitamin D status modifies these results is unknown. The ongoing multicenter (15 sites) RCT using vitamin D3 will be carried out with the number of patients recalculated from the data provided by the original pilot findings.
Treatment trials may be challenging to detect a signal for vitamin D supplementation in severe COVID-19 for two reasons:
- Patients tend to present to hospital in the hyperinflammatory stage of disease, so it might be too late to gain benefit from antiviral effects induced by vitamin D supplementation.
- It is hard to show effects of micronutrients above pharmacology agents, such as dexamethasone, which has potent anti-inflammatory actions and now represents the same standard of care in severe disease.
As shown in many vitamin D supplementation trials, for various outcomes, response and improved outcomes is most observed in those with low baseline 25(OH)D concentrations.
Precarious advice about very high and potentially harmful vitamin D supplementation, which lacks an evidence base, has been circulating during the pandemic and scientific communications should take effort to address such misinformation. This is described in more detail in this piece by Prof. Susan Lanham-New and collegues.
Concluding Thoughts: Pragmatic Steps
Whilst the evidence for vitamin D supplementation in the prevention of SARS-COV-2 infection or severity of outcomes in patients is lacking, many efforts have been made to better understand how vitamin D strategies could be utilised to offset some of the clinical consequences. Irrespective of the strength of evidence, or the COVID-19 pandemic, vitamin D deficiency continues to be a public health issue, particularly of older adults, institutionalised elderly, persons with obesity, and black and Asian ethnic groups. The low costs of vitamin D and its general safety, support arguments for population-level supplementation, perhaps for targeting groups at high risk for vitamin D deficiency and/or COVID-19.
In October 2020, 2.7 million people in England (those on the COVID-19 clinically extremely vulnerable list) were offered free daily vitamin D supplements containing 10 microgram (400IU) for the winter months by the UK government. This vulnerable group are encouraged to ‘opt-in’ as they are likely to have been indoors more than usual, as recommended by protective COVID-19 health measures, so might not have been able to obtain enough vitamin D from sunlight. The existing government advice in the UK, and many European countries is for everyone to take a vitamin D supplement during the winter months. Many population-based studies continue to report low vitamin D supplement use. Vitamin D fortification policies are still under (long and extended) debate.
Summary of Key Points
- The active form of vitamin D, 1,25(OH)2D3, plays many important roles around the body.
- There is an overlap between risk factors for severe COVID-19 and vitamin D deficiency.
- There are plausible mechanisms on which to suspect vitamin D metabolites could exert antiviral effects in the early stages of being exposed to SARS-COV-2, and/or during later phases of actual COVID-19 disease state.
- In relation to observational studies, there is encouraging data but overall the evidence is still conflicting.
- Mendelian randomization studies have thus far shown that genetically lower vitamin D status is not causally associated with COVID-19 susceptibility, severity or hospitalization.
- Trials of vitamin D supplementation have shown mixed results. But such treatment trials may be challenging to detect a signal for vitamin D supplementation in severe COVID-19 for a number of reasons. In general, as is the case for other health outcomes, it is likely that response and improved outcomes will be most observed in those with low baseline 25(OH)D levels.
- Vitamin D deficiency continues to be a public health issue, particularly of older adults, institutionalised elderly, persons with obesity, and black and Asian ethnic groups.
- Currently, the evidence for vitamin D supplementation as an intervention doesn’t have clear and robust evidence to support it. However, despite the evidence strength, given the low costs of vitamin D and its general safety, good arguments could be made for population-level supplementation, particularly targeting groups at high risk for vitamin D deficiency and/or COVID-19.
